

Linking defect
The following 35-year-old male patient with no relevant medical history was referred to us with both maxillary canines impacted and temporary tooth #63 having been weeping for some time following a fistula.
Normally, we could resolve this case by first performing extraction surgery of both canines – the definitive and the temporary, then a second operation for reconstruction of the defect, and a third operation for placement of the implant. This would subject the patient to a greater number of interventions and would treble the time taken for treatment.
We opted to resolve the situation in a single operation. We proceeded to extract the definitive canine, which left an extensive bone defect. Once removed, we detached from the buccal bone where we observed fenestration which left the fistulous tract, and we encountered a linking palate-vestibular-crestal defect.
To resolve this situation, we first placed the implant in its ideal position, emerging through the cingulum, so that our prosthodontist colleague could place screws or cement as he wished.
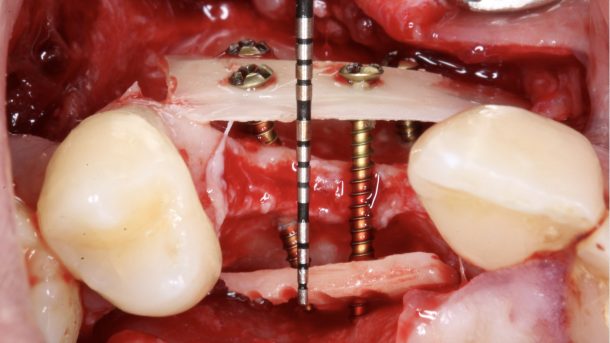
Once this was done, we proceeded to reconstruct the defect with a cortical autograft of bone from the retromolar area of the left mandible. We filled in all defects with particulate autologous bone and closed the reconstruction by fixing a laminate graft.
Below, you can view photographs of the whole surgery up to the placement of gum formers, at which point we referred the patient to our dentistry and prosthodontist colleague.
-


- Previous situation
-
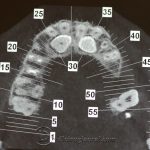
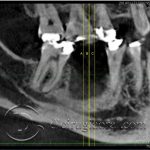
- CT
-

- CT
-

- CT

-

- Before removing the canine
-

- Defect after extraction
-

- Vestibular fenestration due to fistula
-

- Defect communication
-

- Placement of implant
-

- Palate defect
-

- Filling in the defect
-

- Fixed cortical graft
-

- Palate graft filling
-

- Occlusal view
-

- Sutures
-

- Situation after 4 months
-

- Gum former in place
Click to rate this post!
[Total: 0 Average: 0]





Enhorabuena por el resultado. A los 4 meses el aspecto de los tejidos blandos es espléndido. En mi consulta, la verdad es que lo hubiéramos realizado en dos fases, con lo cual ha ahorrado considerablemente fases quirúrgicas y ha acortado el tiempo de tratamiento al paciente. Imagino que luego le colocarían un puente de fibra de vidrio tipo Ribbond al paciente porque no quisieron colocar un pilar provisional sobre ese implante. No?
Estimada Ana,
Gracias por tu comentario. Como bien dices esta cirugía se suele realizar en dos tiempos. Nosotros solemos hacerlo en una cirugía si conseguimos una buena estabilidad primaria en el implante.
Si no me equivoco, pues nosotros no hacemos la prótesis, el paciente no quiso llevar ningún provisional durante los 4 meses de osteointegración fecha tras la cual le realizaron, por fin, la caries del lateral y la corona sobre implantes del canino.
Si te refieres a si hicimos carga inmediata la respuesta es no, pues en un implante con un injerto tan grande la estabilidad se consigue en los 3-4 mm apicales y es un riesgo hacer una carga inmediata que puede comprometer la osteointegración del mismo.
Un saludo