
Quieres leer este artículo en Español? Pincha aquí!
Nowadays a tremendous number of implants are being placed, unfortunately some of these implants might be receiving forces for which they are not prepared to. Among many reasons, two of the most important ones are a bad choice of implant diameter or a disadapted or “not enough” planned prosthetical treatment.
Fractured Implant

Excessive forces in an implant, may lead to abutment loosening, and if this happens and it’s not solved, the abutment screw or even the implant connection itself, may fractured, with the huge problem this situation might be.
In the unlucky event that the implant fractures, makes the situation a lot worse, because there is no other option but to remove the implant.
The explantation or implant removal can be a nightmare, especially if it is fully osseointegrated into the bone.
There are some companies that have launched an implant removal kit, that may give us a little view of this huge problem. But, if the connection, inner part of the implant, is broken, it will greatly limitate the explantation even with removals kit (Bear in mind that most of them use the implant conection to apply explantation forces).
Clinical Case
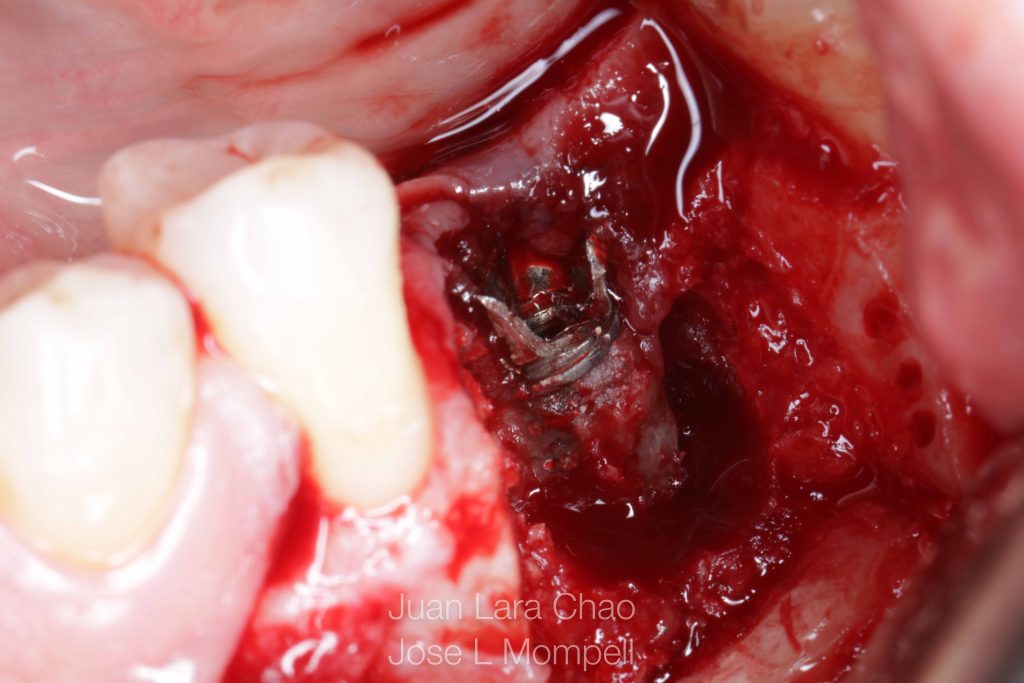
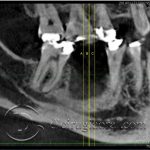
Today, We present a case of a patient who comes to our office with fracture implant wall and its connection located in a very cortical mandibular bone.
We discard the use of removal kits because the connection is very damaged. At this point another solution that have been proposed by different authors is the use of a trephine that has to have a larger diameter that the implant that we need to remove and use it to extract the implant surrounded by the bone that holds it.
In this very case, we have a 4.2x10mm implant. and that means that We would have to use a trephine of internal 5mm internal diameter and 6 mm external diameter. This procedure would leave us a bone defect of at least 6mm diameter and 10-11 millimeters in depth. This large defect, could be difficult to graft and that would condition the whole treatment plan. We might have to graft the area, wait some months for vascularization that and replace the implant. That is why “thinking outside the box” We choose another solution.
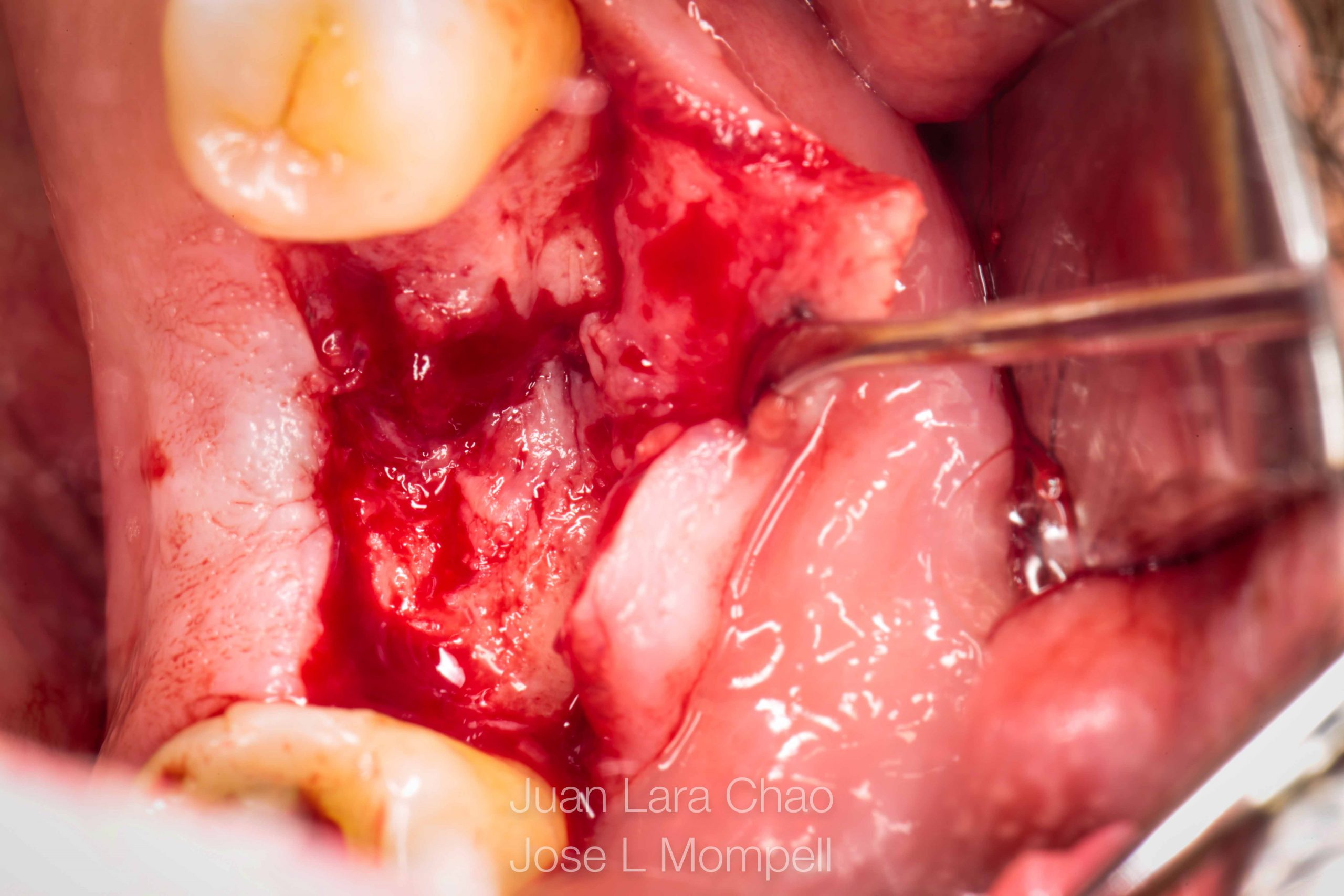
Bone window approach in order to remove the fractured implant
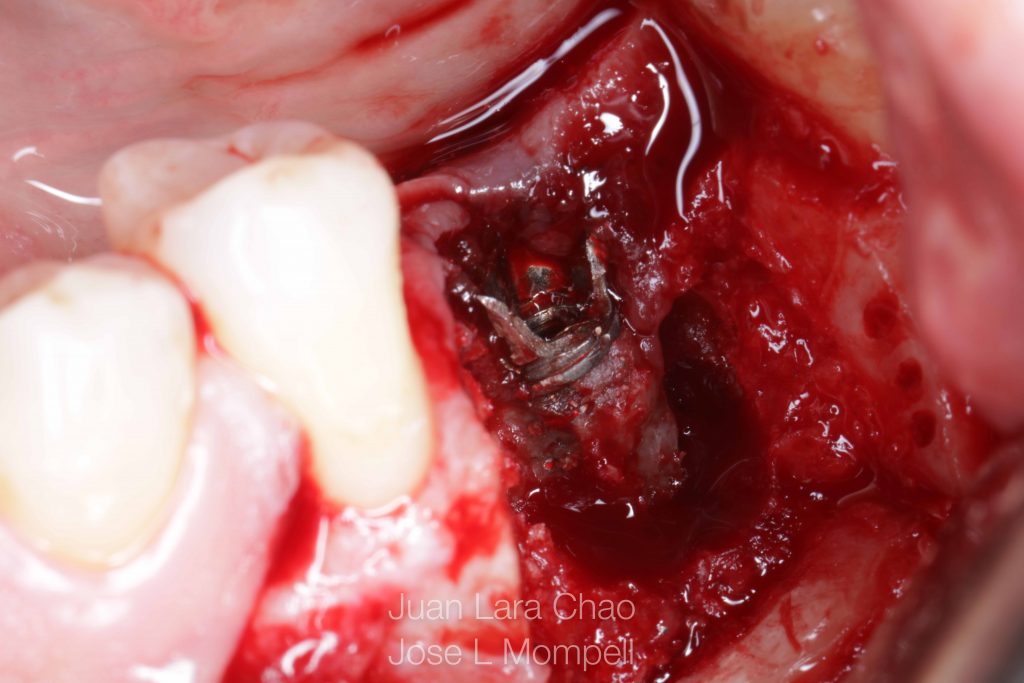
To solve the case in one single surgery and as atraumatically as possible, we choose to perform a bone window with very thin osteotomies.
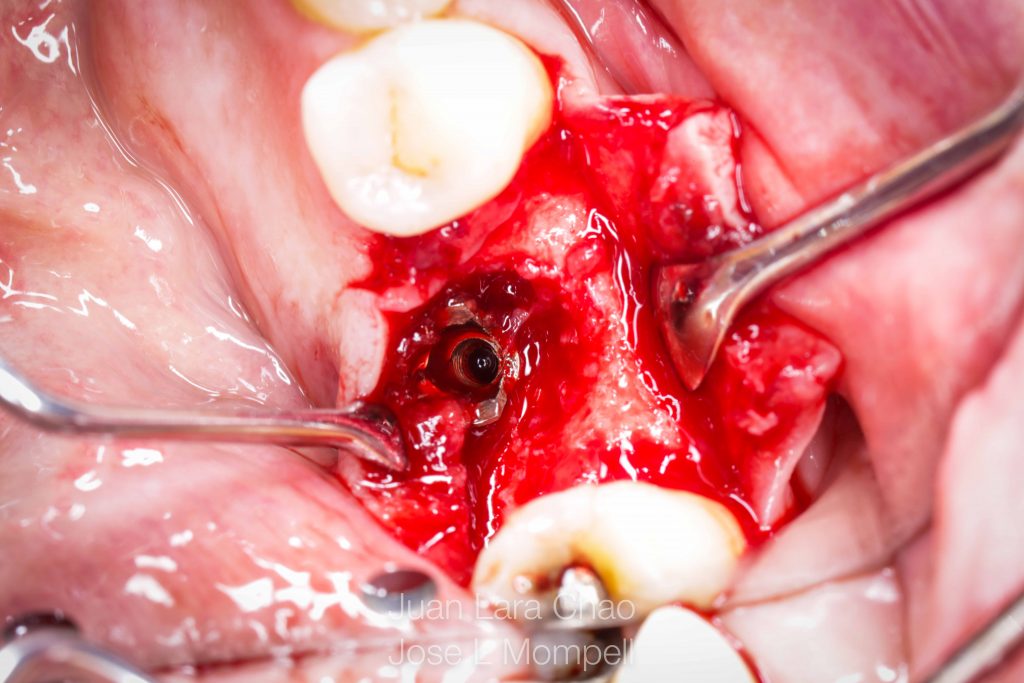
Mandibular buccal bone wall is removed with the use of the microsaw (Creating our window approach into the mandibular medular bone where the fractured implant is located) once removed, we can extract the fractured dental implant and place another implant in the same site.
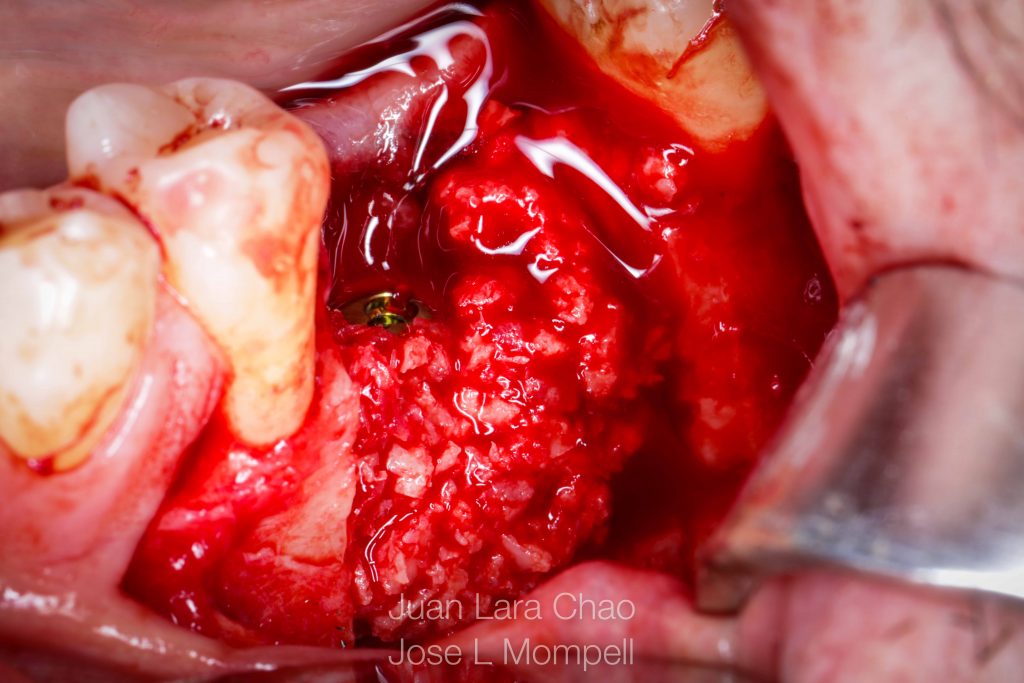
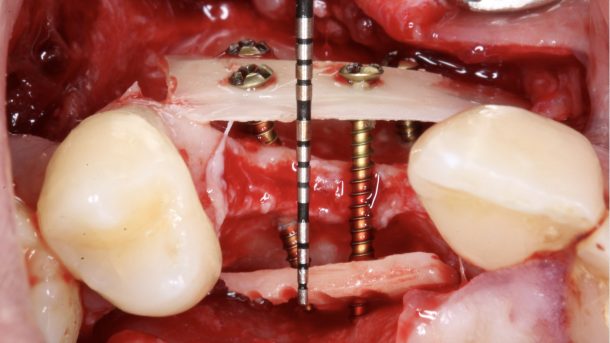
Finally, it will only be necessary to adapt this removed buccal window. To do so, we are going to follow the Split Bone Block tehnique philosophy, proposed by Professor Fouad Khoury.
Based on preventing long-term resorption and accelerating bone vascularization We are going to Split the bone block (Bone window) into two thin bone blades, fixing one of them with two microscrews, rebuilding the bucal missing wall and filling all gaps with particulated bone.
We only wait 16 weeks to perform the second stage surgery or placement of the healing cup. At this moment you can see the great aspect of the bone surrounding the implant, this is when we send our patient to the referral prosthodontist to elaborate the final prosthetic restoration. Xray of the final restoration can be seen in the last picture.
Here you have all pictures of the process, hope you like it!














Trackbacks/Pingbacks